
Published in Astro Awani, Business Today & The Malaysian Medical Gazette, image by Astro Awani.
An understanding of when the daily infection is at its peak in relation to the concept of the flattening of the curve on the spread of Covid-19 will throw some lights on what wave of the pandemic we are at, and what are to be done in facing the current fourth wave of infections.
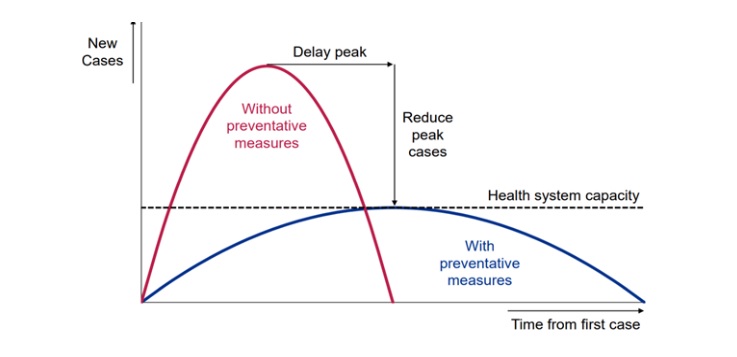
Flattening of the infection curve means reducing the number of infections by influencing its transmission rate via controlling the virus reproduction rate (R nought) through preventative measures of reducing social contacts such as the MCO, and at the same time upgrading the capacity of the healthcare system to cope with an increasing number of infections.
The result – the number of infections will peak early as shown by the blue flattened curve in the diagram below with relatively fewer cases compared to a scenario without any intervention (red curve) at all.

What the graph is telling us is, there are two phases of the flattening of the curve. The first phase of flattening of the curve occurs when the daily infection figure reaches its peak. At this stage the curve will plateau (flatten). The curve cannot flatten for as long as the peak is not reached.
When the observance of the MCO “culture” which indicates social responsibility of the rakyat is in action and becomes the salient feature of the MCO – such as observing social/physical distancing, practising regularly personal hygiene like washing hands, avoiding large gathering and wearing a mask in public – a second phase of flattening of the curve to its floor as shown in the diagram, which will then taper to a zero infection will occur.
In Malaysia, the first wave of the Covid-19 pandemic last year began from Jan 25 to March 2. On Jan 25, Malaysia announced its first three cases of Covid-19. The peak daily infection for this first wave was recorded on Feb 8 with four cases. The infection curve started to flatten to its floor with zero cases for 11 consecutive days beginning Feb 16, indicating the ending of the first wave.
On Feb 27, these zero cases came to an end but because the new cases from that day until March 2 did not breach the peak of four cases, at this stage it was still the first wave.
The second wave began on March 3 with seven cases, breaching the peak of the first wave (4), and ended on Oct 1 (260 new cases). Soon after the daily infection recorded a three-digit figure for the first time ever on March 15 with 190 cases, MCO 1.0 was announced by the government, effective from March 18.
The peak for this second wave was recorded at 277 cases on June 4. Since then, the curve has flattened, with new daily cases thereafter going up and down like a yoyo where there are instances of a one-digit daily infection for some days. But when it went up, it never breached the peak of 277 cases. This second wave never witnessed the second phase of the flattening of the curve to its floor (zero cases).
On Oct 2, the third wave began with new cases at 287, breaching the peak of the second wave (277). The peak of the third wave was 5,728 new cases recorded on Jan 30 this year. The third wave ended on May 18 with 4,865 new cases without flattening of the curve to its floor (zero cases), as in the second wave.
On May 19, we saw new cases at 6,075, breaching the peak of the third wave and signalling the start of the fourth wave. Has the fourth wave reached its peak? The dicey thing about determining the peak is, it is only known in hindsight.
When the peak of the second wave was recorded at 277 cases on June 4 or the peak of the third wave on Jan 30 (5,728), no one knows on that day that this number was going to be the peak.
But having a rough idea of when the peak will be reached is important because it gives us a clue to the flattening of the infection curve or at least give us a sense of relief that the worst is over (without any implication that we are out of the woods).
Today (June 1) we are on the 14th day of the fourth wave. So far, the highest daily infection recorded within these 14 days is 9,020 cases on May 29. Could this be the peak especially after a drastic drop in the next two days of 6,999 (May 30) and 6,824 yesterday (May 31)? Hopefully so, although we can’t be certain.
However, from studying the pattern of the previous waves, we know that the peak in the first wave was reached 14 days after Covid-19 made its appearance in this country; the peak of the second and third waves were both reached three months after each wave began. In term of duration, the first wave lasted for one month and six days; the second wave, seven months; and the third wave, seven months and 16 days.
This tallies with science which says subsequent waves will be more lethal, infectious and take relatively longer time to end because of the various mutations of the virus which lead to the emergence of various tough variants.
But what is of concern here is that even if preventative measures in the MCO are there, the path to a flattening of the curve will be longer if the capacity of the healthcare system is not upgraded.
With intervention in the form of an urgent upgrading of the capacity of the healthcare system, more ICU wards, more quarantine spaces, more ventilators, more equipment for testing and screening, and more protective gear for the frontline doctors and nurses can be provided, which in turn will ensure the number of infected people getting the needed medical attention will increase, thereby increasing the recovery rate and reducing the fatality rate, all these under a scenario of a two percent case fatality rate, ceteris paribus – everything else remain constant.
This in turn will give some breather for “regrouping” by allowing some frontline doctors and nurses to rest, reducing further the number of infections among healthcare workers at the frontline.
A proviso though: unlike in economic theory, in real life ceteris is not paribus and in the absence of other preventative measures, like the implementation of the current Full MCO (FMCO), this breather which is a narrow window of opportunity, will deteriorate soon enough because it is also a breather for the remaining Covid-19 virus to buy time and fortify themselves via more mutations for another wave of attack.
Judging by Prime Minister Muhyiddin Yassin’s speech yesterday when he unveiled a RM40b Pemerkasa Plus in economic aid, which includes RM5 billion direct fiscal injection from the federal government where quite a huge chunk of it went to the Health Ministry for upgrading the capacity of the healthcare system, he is indeed moving in the right direction, making Malaysia a good model for countries which were late in taking such action because of bureaucratic paralysis.
Among the action taken to boost public healthcare capacity:
- RM450m to increase hospital beds and procure equipment for intensive care units, including at teaching hospitals of public universities at military field hospitals;
- RM550 million for spending related to Covid-19 including increased operating and management expenses, procurement of medicines and reagents, and appointment of contract officers; and
- Extend the service of 14,000 contract medical officers and nurses until 2022, and appoint 500 healthcare workers who are due for mandatory retirement this year on a contract basis.
Hopefully, the brief respite afforded to us due to these preventative actions of an FMCO and the upgrading of the healthcare system can extend a little bit further the respite by shortening the time taken for the curve to reach its peak and also the duration of the fourth wave.
But the saving grace to all this is the vaccination programme being carried out now that will just speed up the discovery process of the peak and shorten the duration of the current wave via herd immunity. Also, who knows during this respite, an important approved drugs that can cure Covid-19 will emerge, which will further flatten the curve to the floor.
And here’s where the government needs your help. Whether you are in the frontlines of the battle – healthcare and essential services manpower – or behind the lines, each one of us have a duty to perform: those at the frontlines are working for the sake of those staying at home during FMCO, and those behind the lines must stay at home as much as possible during the FMCO for the sake of those working at the frontlines.
Jamari Mohtar is Director, Media & Communications at EMIR Research, a think tank focused on strategic policy recommendations based on rigorous research.
Diterbitkan di Agenda Daily & Malaysiakini.
Pemahaman tentang bila kah jangkitan harian berada di puncaknya berhubung dengan konsep melandaikan lengkung penularan Covid-19 akan memberikan kita gambaran mengenai tahap gelombang pandemik yang sedang kita hadapi, dan apa yang harus dilakukan dalam menghadapi gelombang keempat jangkitan ketika ini.
Melandaikan lengkung jangkitan bermaksud mengurangkan jumlah jangkitan dengan mempengaruhi kadar penularannya dengan mengawal kadar pembiakan virus (R naught) melalui langkah-langkah pencegahan mengurangkan kontak sosial yang terdapat dalam Peraturan Kawalan Pergerakan (PKP), dan pada masa sama meningkatkan keupayaan sistem penjagaan kesihatan untuk menangani peningkatan jumlah jangkitan.
Hasilnya – jumlah jangkitan akan memuncak lebih awal seperti yang ditunjukkan oleh lengkung biru dalam rajah di bawah dengan kes jangkitan yang lebih rendah berbanding dengan senario tanpa langkah-langkah pencegahan sama sekali (lengkung merah).
Berdasarkan graf di atas, terdapat dua fasa melandaikan lengkung. Fasa pertama berlaku apabila angka jangkitan harian mencapai puncaknya. Pada tahap ini lengkung akan melandai (mula merata tanpa begitu curam). Lengkung tidak dapat dilandaikan selagi jangkitan harian belum berpuncak.
Apabila pematuhan “budaya” PKP yang menunjukkan tanggungjawab sosial rakyat menjadi ciri utama PKP – seperti mematuhi penjarakan sosial/fizikal, mengamalkan kebersihan diri secara berkala seperti mencuci tangan, mengelakkan perhimpunan besar dan memakai pelitup muka di khalayak ramai – fasa kedua melandaikan lengkung hingga ke lantai graf akan berlaku seperti yang ditunjukkan dalam rajah, yang kemudiannya akan meruncing ke arah jangkitan sifar.
Di Malaysia, gelombang pertama pandemik Covid-19 tahun lalu bermula pada 25 Januari hingga 2 Mac. Pada 25 Januari, Malaysia mengumumkan tiga kes pertama Covid-19. Puncak jangkitan harian gelombang pertama ini dicatatkan pada 8 Februari dengan empat kes. Lengkung jangkitan mula melandai ke lantai dengan kes sifar selama 11 hari berturut-turut bermula pada 16 Februari, menandakan berakhirnya gelombang pertama.
Pada 27 Februari, kes sifar ini berakhir tetapi kerana jumlah kes baru dari hari itu hingga 2 Mac semuanya berada di bawah empat kes (puncak jangkitan), ia masih merupakan gelombang pertama.
Gelombang kedua bermula pada 3 Mac dengan tujuh kes, mengatasi puncak gelombang pertama (4), dan berakhir pada 1 Oktober (260 kes baru). Sejurus selepas jangkitan harian mencatatkan angka tiga digit untuk pertama kalinya pada 15 Mac dengan 190 kes, PKP 1.0 diumumkan kerajaan, berkuat kuasa pada 18 Mac.
Puncak bagi gelombang kedua ini dicatat pada 4 Jun dengan 277 kes. Sejak itu, lengkung semakin melandai, dengan kes harian baru selepas itu turun naik bagaikan permainan yo-yo di mana terdapat kejadian jangkitan harian satu digit selama beberapa hari.
Tetapi ketika ia meningkat, jangkitan harian tidak melebihi puncak 277 kes. Gelombang kedua ini tidak pernah menyaksikan fasa kedua lengkung melandai ke lantai (kes sifar).
Pada 2 Oktober, gelombang ketiga bermula dengan 287 kes baru, menembusi puncak gelombang kedua (277). Puncak bagi gelombang ketiga adalah 5,728 kes baru yang direkodkan pada 30 Januari tahun ini. Gelombang ketiga berakhir pada 18 Mei dengan 4,865 kes baru tanpa menyaksikan pelandaian lengkung ke lantai (kes sifar), seperti juga pada gelombang kedua.
Pada 19 Mei, kes baru berjumlah 6,075, menembusi puncak gelombang ketiga yang menandakan permulaan gelombang keempat. Adakah gelombang keempat telah mencapai kemuncaknya? Puncak gelombang sebenarnya sukar ditentukan serta merta kerana ia hanya diketahui kemudian.
Umpamanya, ketika puncak gelombang kedua dicatat pada 277 kes pada 4 Jun atau puncak gelombang ketiga pada 30 Januari (5,728), tiada seorang pun yang tahu pada hari tersebut jumlah itu akan menjadi puncak.
Tetapi mempunyai idea kasar tentang bilakah puncak jangkitan akan dicapai adalah penting kerana ia memberi kita petunjuk mengenai pelandaian lengkung jangkitan atau sekurang-kurangnya memberi kita kelegaan bahawa keadaan terburuk sudah berakhir (tanpa implikasi bahawa masalah telah berakhir).
Semalam (1 Jun) kita berada pada hari ke-14 gelombang keempat. Setakat ini, jangkitan harian tertinggi yang dicatatkan dalam 14 hari ini adalah 9,020 kes pada 29 Mei. Mungkinkah ini merupakan puncak bagi gelombang keempat terutama selepas penurunan drastik dalam dua hari berikutnya iaitu 6,999 kes (30 Mei) dan 6,824 kes dua hari lepas (31 Mei)? Mudah-mudahan begitu, walaupun sukar untuk dipastikan.
Namun, berdasarkan corak gelombang sebelumnya, kita tahu puncak gelombang pertama dicapai 14 hari setelah Covid-19 muncul di negara ini; puncak gelombang kedua dan ketiga, kedua-duanya dicapai tiga bulan selepas setiap gelombang bermula. Dari segi jangka masa, gelombang pertama berlangsung selama satu bulan, enam hari; gelombang kedua, tujuh bulan; dan gelombang ketiga, tujuh bulan, 16 hari.
Ini sejajar dengan sains yang mengatakan gelombang susulan akan menyaksikan lebi banyak korban jiwa, penularan tegar jangkitan dan memakan masa yang lebih lama untuk berakhir kerana pelbagai mutasi virus yang menyebabkan munculnya pelbagai varian.
Tetapi yang penting di sini ialah walaupun terdapat langkah pencegahan PKP, jalan menuju melandaikan lengkung akan lebih berpanjangan sekiranya kapasiti sistem penjagaan kesihatan tidak ditingkatkan.
Dengan campur tangan dalam bentuk peningkatan mendadak kapasiti sistem penjagaan kesihatan, lebih banyak wad ICU, lebih banyak ruang kuarantin, lebih banyak kelengkapan pernafasan (ventilator), lebih banyak peralatan untuk ujian dan saringan dan lebih banyak kelengkapan pelindung untuk doktor dan perawat barisan depan dapat disediakan.
Ini semua akan memastikan bilangan orang yang dijangkiti mendapat rawatan perubatan yang diperlukan akan meningkat, lantas meningkatkan kadar pemulihan dan mengurangkan kadar kematian, di bawah senario kadar kes kematian 2%.
Ini kemudiannya boleh memberi nafas untuk “berkumpul semula” dengan membolehkan beberapa doktor dan jururawat barisan depan berehat, sekali gus mengurangkan lagi jumlah jangkitan di kalangan pekerja kesihatan di barisan depan.
Namun, jika tidak ada langkah pencegahan lain, seperti pelaksanaan PKP Menyeluruh (PKPM) yang kini dilaksanakan, peluang sempit untuk bernafas ini akan menjadi lebih sempit kerana ia juga merupakan peluang sempit bernafas bagi virus Covid-19 yang tersisa untuk membeli masa membentengi diri melalui lebih banyak mutasi untuk gelombang serangan yang seterusnya.
Berdasarkan ucapan Perdana Menteri Muhyiddin Yassin dua hari lepas (31 Mei) ketika melancarkan Pemerkasa Plus bernilai RM40b dalam bentuk bantuan ekonomi yang merangkumi suntikan fiskal langsung RM5b dari kerajaan persekutuan di mana sebahagian besar peruntukan adalah untuk Kementerian Kesihatan meningkatkan kapasiti sistem penjagaan kesihatan, beliau sememangnya bergerak ke arah landasan yang betul, menjadikan Malaysia model yang baik bagi negara-negara yang terlambat mengambil tindakan tersebut kerana kelumpuhan birokrasi.
Antara tindakan yang diambil untuk meningkatkan keupayaan penjagaan kesihatan awam:
• RM450j untuk menambah katil hospital dan mendapatkan peralatan untuk unit rawatan rapi, termasuk di hospital perguruan universiti awam di lapangan hospital tentera;
• RM550j untuk perbelanjaan yang berkaitan dengan Covid-19 termasuk peningkatan perbelanjaan operasi dan pengurusan, perolehan ubat-ubatan dan reagen, serta pelantikan para pegawai
kontrak; dan
• Memperpanjang perkhidmatan 14,000 pegawai perubatan dan jururawat kontrak sehingga 2022, dan melantik 500 pekerja penjagaan kesihatan yang dijadualkan bersara wajib tahun ini berdasarkan kontrak.
Mudah-mudahan, peluang sempit yang singkat ini dengan adanya tindakan pencegahan PKPM dan peningkatan kapasiti sistem penjagaan kesihatan dapat memperpanjang sedikit masa jeda dengan memendekkan masa yang diperlukan untuk lengkung mencapai puncaknya dan juga jangka masa keempat gelombang.
Tetapi rahmat yang tersimpan dalam hal ini adalah program vaksinasi yang dilakukan sekarang yang akan mempercepat proses penemuan puncak dan memendekkan jangka waktu gelombang keempat melalui imuniti kelompok.
Juga, siapa tahu semasa peluang sempit ini, ubat-ubatan penting yang dapat menyembuhkan Covid-19 akan muncul, yang kemudiannya akan melandaikan lengkung ke lantai (kes sifar).
Di sinilah kerajaan memerlukan bantuan anda. Sama ada anda berada di barisan depan pertempuran – sebagai tenaga kerja kesihatan dan perkhidmatan penting – atau di belakang garisan, setiap kita mempunyai tugas: mereka yang berada di barisan hadapan bekerja untuk kepentingan mereka yang tinggal di rumah semasa PKPM, dan mereka di belakang garisan mestilah tinggal di rumah sebanyak mungkin semasa PKPM demi kepentingan mereka yang bekerja di barisan hadapan.
Jamari Mohtar adalah Pengarah, Media & Komunikasi di EMIR Research, sebuah organisasi pemikir bebas yang berfokuskan kepada pencernaan saranan-saranan dasar strategik berteraskan penyelidikan yang terperinci, konsisten dan menyeluruh.

