Published by EMIR Research, image from Malaysiakini.
Prime Minister Muhyiddin Yassin actually did not mince words when he said in his address to the nation that the movement control order (MCO) could be terminated by the end of this month, provided that all Malaysians give their full cooperation to it by staying at home in order to reduce the number of infections.
With more or less one week to go, is this a pipe dream, notwithstanding that it could be extended as explained by the PM if the numbers do not show significant improvement?
I don’t think so. There is a big possibility that the MCO might be terminated, provided with the cooperation of the rakyat to stay at home, a magic number in daily infection is arrived at, by the end of the MCO which has been crunched by policy wonks in the government. I will touch on this magic number later.
If in my previous article, flattening of the curve means reducing the number of infections by influencing its transmission rate via controlling the effective reproduction rate (R) through social distancing measures like MCO, this time around the curve can also be flattened by upgrading the capacity of the healthcare system to cope with an increasing number of infections.
The theory behind this is depicted in the graph below.
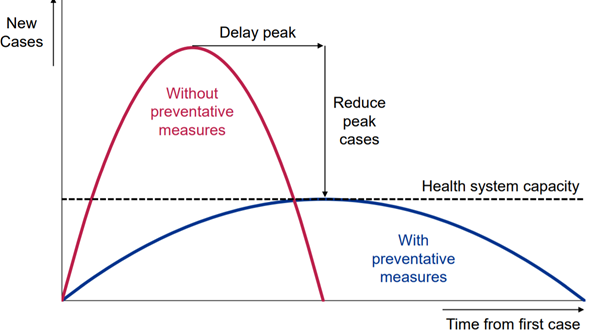
What the graph is saying is that when intervention in the form of an urgent upgrading of the capacity of the healthcare system, represented by the dotted horizontal line, is done, more ICU wards, more quarantine spaces, more ventilators, more equipment for testing and screening, and more protective gear for the frontline doctors and nurses, the curve will flatten or plateau as compared to the second curve where there is no intervention at all in the form of preventative measures such as social distancing to cope with Covid-19.
The result – the number of infections will peak early as shown by the flattened curve with relatively fewer cases compared to a scenario without any intervention at all.
This also means the number of infected people getting the needed medical attention will increase, thereby increasing the recovery rate and reducing the fatality rate, all these under a scenario of a 2% case fatality rate, ceteris paribus – everything else remain constant.
This in turn will give some breather to the affected country to “regroup” by allowing some frontline doctors and nurses to rest, reducing further the number of infections among healthcare workers at the frontline.
Judging by Muhyiddin’s speech where quite a huge chunk of the budget went to the Health Ministry for upgrading the capacity of the healthcare system, he seems to be moving in this direction and that is indeed the right direction, making Malaysia a good model for countries which were late in taking such action because of bureaucratic paralysis.
In fact, the DG of Health, Dr Noor Hisham Abdullah, has paved the way for PM’s announcement when on March 22, he declared the Health Ministry expects to be able to carry out 16,000 Covid-19 screenings a day by April compared to just 3,500 now (surprise, surprise April, and 31 March is just one day before April).
“Tests are currently being conducted by 18 Health Ministry and five private laboratories. The Institute for Medical Research will train several other laboratories, including in military and university hospitals, to enhance Malaysia’s ability to conduct Covid-19 detection tests,” he added.
More nurses will be deployed in states with a very high number of Covid-19 patients, along with recalling of retired specialist doctors and nurses for duties.
The ministry is also cooperating with private hospitals to jointly tackle the health problem. Out of 148 ministry hospitals, 26 have been identified to be used to treat Covid-19.
The government has also prepared 3,400 beds in the 26 hospitals, with 300 units of ICU for Covid-19 cases. There are also currently 925 ventilators available although 500 more are needed. If the ICU is full, isolation wards can be used because ventilators are still available.
Currently, 18 percent of the ICU units are being used while 20 percent of the 3,400 beds are occupied. Clearly, the government is taking steps to prevent the healthcare system from being overwhelmed with Covid-19 pandemic.
A proviso though: unlike in economic theory, in real life ceteris is not paribus and in the absence of other preventative measures, this breather which is a narrow window of opportunity, will deteriorate soon enough because it is also a breather for the remaining interim weakened Covid-19 virus to buy time and fortify themselves for a second wave of attack.
This new wave of attack will be more menacing, causing the plateaued infections to increase again. The curve after plateauing will thus rise again because of these new infections.
Hence, to ensure the thorough success not only in this upgrading of the capacity of the healthcare system which includes its manpower too that must be properly and efficiently trained to fight the Covid-19 virus according to the most intelligent and dynamic battleplan, the current MCO must also be implemented with efficiency and perfect precision so that the upgrading of healthcare system can begin on a smooth footing.
By smooth footing, I mean while the virus is buying time (which is relatively brief) to fortify themselves for a new attack, quarantine and ICU wards in hospital and clinics should be reserved for those with underlying health problems. The conspiracy theorists among us will definitely associate those with underlying symptoms as the elderly who is above 80 – our granny and nanny.
But look at the statistics, those with underlying health problems could be someone in their mid-30 to 50s. Cancer, heart attacks, hypertension are all diseases of an affluent society where the victims are getting younger and younger. Even those in their 20s could die of cancer and heart attacks.
So, regardless of age those who are healthy and without symptoms but are close contacts of the infected, discovered via contact tracing should quarantine themselves for 14 days at home in a room by themselves with minimal contacts with family members.
And here’s where the government needs your help. Whether you are in the frontlines of the battle – healthcare and essential services manpower – or behind the lines, each one of us have a duty to perform: those at the frontlines are working for the sake of those staying at home during MCO, and those behind the lines must stay at home during MCO for the sake of those working at the frontlines.
I’m just paraphrasing a slogan which has become a popular hashtag during the MCO.
Hopefully, the brief respite afforded to us due to these unique preventative actions of MCO (our MCO is different from the Wuhan and Italy’s lockdown models) and upgrading instantly our healthcare capacity can extend a little bit further the respite. Who knows during this “lengthened” respite, an important approved drugs or vaccine will be readied to inoculate those infected and quarantined, which will further flatten the curve to the floor.
At the beginning of this article I mentioned about a magic number on the daily infections that will make the government lift the MCO. What is that number? Obviously, it should be a number that is as low as possible and wherewith the number is seen by the policymakers as one that will put the second phase of the battle plan into action on a firm and sound footing – the mitigation part i.e. upgrading the capacity of the healthcare system. Otherwise brace ourselves for a long stay at home.
And before I end, an explanation on the heading of my article which ends in question mark. It simply means whether Malaysia will become a model in its fight against the virus does not solely depend on the government. We too have a stake in determining a happy ending to the Covid-19 saga. Can we do it?
And let us not be pessimistic. The Wuhan model which is very severe and draconian in its lockdown, began with more than 4,000 daily infections just a week after lockdown on Jan 23 – representing a 30% daily increase which is exponential.
At this rate, according to Nobel Laurette Michael Levitt, each and every one of the Wuhanis were theoretically at risk of becoming infected. Turned out only 3% were infected.
And what’s interesting is two weeks after the lockdown, although the number is still high, there was actually a consistent daily drop in the number of infections which continues for weeks, signifying a change from an exponential increase to a linear one. Two weeks after this drop, it is the turn of the fatality rate to drop though in absolute term it’s still quite high. Note another magic number – two weeks (that’s why the MCO is two weeks to begin with, and if it’s extended it will be on a two week basis for each extension).
By early March, there were instances of a nil infection in a day at first sporadically and then consistently till today. Although China has not declared it’s free from the Covid-19 pandemic, many experts believe she is on the way there by the end of March.
What accounts for this “fast” recovery? Professor Levitt thinks besides lockdown (social distancing) and upgrade of the capacity of the healthcare system, the natural immunity of humanity also plays a part. I don’t want to touch at length on this lest those on the fringes will advocate sacrificing children and the elderly (those above 80) – to the infection for the sake of economic survival of the nation.
Yes, lockdown or MCO cannot be the long-term answer because there must be some fine balance between lockdown and economic death but the answer does not lie in sacrificing human lives, even a single human life if we can help it.
So, yes let’s hope the MCO is two weeks. The numbers will get worse before they get better within these two weeks. We can do it. All must cooperate, all must complement each other and finally all must stay at home!
Jamari Mohtar is Director, Media & Communications at EMIR Research, a think tank focused on strategic policy recommendations based on rigorous research.